ELECTROCARDIOGRAM (ECG) &
ASSOCIATED INVESTIGATIONS:
Electrocardiogram
is abbreviated as ECG (though sometimes is seen as EKG taken
from the Greek word 'Kardia') and is the recording of electrical
activity form the heart. It is a simple, painless examination
that takes around 10 minutes to perform.
Electrode
Placement
It
consists of applying 10 leads to the body connected usually to
small adhesive pads (electrodes) that will provide 12 different
recordings of the electrical activity that is given off by the
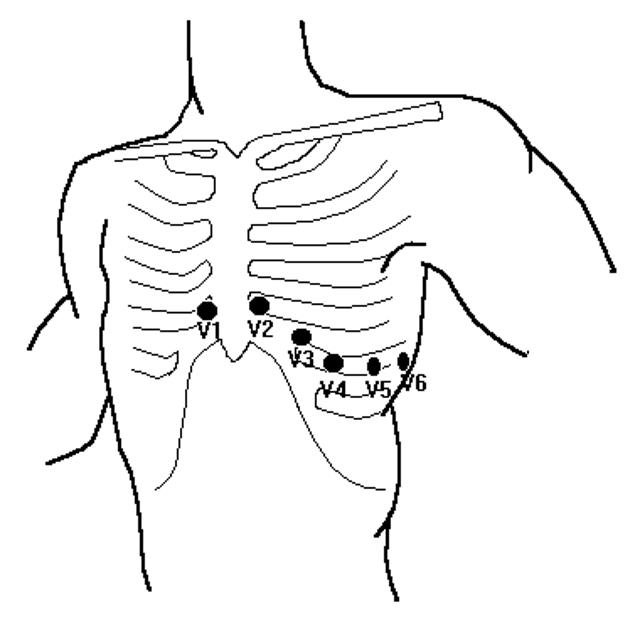
heart. The electrodes are attached on each limb (called the Limb
Leads) and across the left side of the chest (called the V
Leads) in specific positions:
- V1 - In
the 4th intercostal space on the right side of the sternal
border
- V2 - In
the 4th intercostal space on the left side of the sternal
border
- V3 -
Midway between V2 and V4, no anatomical positioning required
- V4 - In
the 5th intercostal space in line with the middle of the
clavicle
- V5 - In
line with the anterior axilla (front of the armpit) in line
with V4
- V6 - In
line with the mid-axilla (middle of armpit) in line with V4
and V5
There
are times when the leads will be placed in different positions
or there may be less or more leads attached:
If
information about the back of the heart (posterior) is required
then the Chest (V leads) may be extended to:
- V7 -
Left posterior axilla in (back of armpit) in line with
V4/V5/V6
- V8 - At
the tip of the scapula (shoulder blade) in line with V7
- V9 -
Left para-spinal region (next to the spine) in line with V8
In
Intensive Care or Cardiac Wards three leads may be attached to
provide basic monitoring information.
In
amputees the limb electrode would be placed as near to the limb
position as possible and this may be on the shoulder or hips.
In
neonate babies the chest wall is so small V3 is omitted and the
chest progression leads begins with V4 on the right side,
denoted V4R, then V1, V2, V4, V5 & V6.
In
a very rare condition called dextrocardia, the Chest leads (V
Leads) may be reversed to cover the right side of the chest
because the heart is transposed, that is a mirror image of the
correct positioning of the heart. So V1 would be in the 4th
intercostal space on the left sternal border and called V1R.
If
Atrial activity is of particular interest a lead placement may
be performed to increase the visibility of the activity. This is
called the Lewis lead or S5, and is created by placing the right
arm lead in the 2nd intercostal space on the right sternal
border and the left arm electrode is placed in the 4th
intercostal space on the right sternal border. The Lewis lead
would then be viewed on Lead 1 of the ECG enhancing the atrial
activity, such as atrial flutter.
Uses
of ECG
The
ECG may only be the starting point for screening and detecting
cardiac problems. There are various other methods or means of
recording the ECG such as:
If ECG
information is required over an extended period of time then
the ECG may be repeated every so often every hour. This would
enable clinicians to monitor any rapidly changing ECG such as
a heart attack 'evolving' and 'resolving'.
If ECG
information is required over a longer period then an
Ambulatory ECG may be performed, this is where the patient is
connected to a small recording device that they take away and
wear for 24 - 72 hours.The ECG is recorded constantly and rate
and rhythm trends are seen and any symptomatic episodes or
abnormalities can be looked at in detail more carefully.
However a person's problems may be more infrequent than every
1-3 days.

If
a patients symptoms are more infrequent then they may be given
a 'Cardio-Memo' device. This device has no leads but is the
size of a mobile phone and is placed on the chest wall when
the person is symptomatic.This reduces the inconvenience of
wearing a device constantly but may miss irregularities that
are not symptomatic or when the subject is asleep.
Cardio-Memo's are given on loan for 3 days or longer or until
the patient captures a symptomatic episode.
An
ECG with Exercise (sometimes called a Stress test or exercise
stress test) may be indicated when the symptoms include chest
pain, breathlessness or palpitations. The ECG is recorded
whilst the person performs exercise that gradually gets more
difficult until they fatigue, become symptomatic or a certain
heart rate is obtained. The exercise may be performed on a
stationary bike or a treadmill, it is also possible to emulate
exercise by using drugs/medication.
 History of the ECG History of the ECG
The
first accurate recording of an ECG was in 1895 and the waveforms
were eventually designated P, Q, R, S and T. Each waveform
is representative of a certain portion of the cardiac cycle or
heart beat. More detailed information can be found in the ECG
Screening Course PDF but simply; the P wave is atrial
contraction (Depolarisation), the QRS is the various parts of
the ventricle contracting (Depolarisation) and the T wave is the
'recovery' (Repolarisation) of the ventricles. Occasionally
there is a further, small wave called the U wave and this is
thought to be the late repolarisation of papillary muscles or
Purkinje fibres.
The information that can be gained from an ECG is taken by
analysing the rate and overall rhythm of the ECG, the morphology
(shape) and measurements of the ECG and by evaluating the timing
of the components of the ECG waveforms.
Artefacts
Care
should be taken when performing an ECG as the recorded waveform
may be contaminated with artefacts. Artefacts can be considered
to be any electrical potentials that do not arise from the heart
or something that affects the portrayal of the true ECG.
The main sources of artefact come from:
- The
recording equipment/leads or electrodes (ECG machine)
- Electrical
interference external to the recorder
- The
patient
- The
Electrocardiographer or person performing the ECG
ECG
Screening Course
|