|
DECREASED SOUND TOLERANCE: HYPERACUSIS,
MISOPHONIA & HYPERSENSITIVITY
- Audiometry
- Tympanometry
- Adv Audiology
- Vestibular
- Allergy Testing
- Tinnitus
- Hyperacusis
- Misc. Audiology
- Clinical Photography
Decreased
sound tolerance, including hyperacusis, misophonia, and phonophobia, is
a challenging topic to study, and a challenging symptom to treat.
Many questions are unanswered; the aetiology is not clear, neural
mechanisms are speculative and treatments are not yet proven.
 There are many
differing terms to name certain conditions relating to a subjective
decreased sound tolerance in people. The terms hypersensitivity,
hyperacusis, recruitment, dysacusis, auditory hyperesthesia,
misophonia, phonophobia and many other terms have been used
indiscriminately to describe conditions relating to any kind of reduced
tolerance to sound or discomfort in the ears with sound exposure. There are many
differing terms to name certain conditions relating to a subjective
decreased sound tolerance in people. The terms hypersensitivity,
hyperacusis, recruitment, dysacusis, auditory hyperesthesia,
misophonia, phonophobia and many other terms have been used
indiscriminately to describe conditions relating to any kind of reduced
tolerance to sound or discomfort in the ears with sound exposure.
Although there is no generally accepted term to describe the various
decreased sound tolerance conditions it must be remembered that this
topic is only recently starting to gain some momentum after the
original work of Jastreboff and other authors. This subject is still
not well researched or documented and for many sufferers, due to a lack
of understanding regarding a firm diagnosis, the causative
pathophysiology and resultant treatment options, patient satisfaction
is often poor.
Clinical research reveals that in many cases, decreased sound tolerance
is a complex phenomenon and frequently consists of multiple conditions.
In some cases, it is not necessarily loud sounds but quiet sounds that
can cause discomfort. It has been recognised that decreased sound
tolerance might reflect a physical discomfort, or can be related to a
dislike or a
fear/anxiety of sound.
A major caveat is that hyperacusis, misophonia or phonophobia does not
necessarily have any relation to hearing thresholds. Patients with
hyperacusis, misophonia or phonophobia may have normal hearing or they
may have some hearing loss. They may also have tinnitus but this is not
exclusive.
From the current literature, the following is the generally accepted
description of each term.
Hyperacusis
Definition:
A simple
definition of hyperacusis is:
An Increased Sensitivity to
Noise.
In more detail, hyperacusis can be defined as an abnormally strong
reaction to sound occurring within the auditory pathways. At a
behavioural level, it manifests by the subject experiencing physical
discomfort because of exposure to sound. This same sound would not
result in a similar reaction to the average person. There is limited
data available regarding the prevalence of decreased sound tolerance.
Cause:
Most
frequently decreased sound tolerance results from a combination of
hyperacusis and misophonia/phonophobia but has been reported as an
isolated finding or as a component of multi-symptom diagnosis.
It is important to assess the presence and the extent of all these
phenomena in each patient, as these phenomena need to be treated using
different methods. Some research shows that hyperacusis and tinnitus
co-exist at the same time. They quote that around 40% of tinnitus
patients exhibit some degree of decreased sound tolerance and that 86%
of subjects questioned with hyperacusis suffered from tinnitus.
Decreased sound tolerance can exist as an independent medical
diagnosis, or may be associated with problems that are more complex.
Medical conditions previously linked to decreased sound tolerance
include: tinnitus, Bell's palsy, Lyme Disease, Williams Syndrome,
Ramsay Hunt Syndrome, ear surgery, perilymphatic fistula, head injury,
migraine, depression, withdrawal from some antidepressants, increased
Cerebral Spinal Fluid pressure and Addison's disease. Hyperacusis
has also been linked to sound exposure (particularly short, impulse
noise), stress and drugs. In some cases, a negative life event appears
to be associated with the onset of hyperacusis as well as children on
the autistic spectrum.
There may be a learned association of fear/anxiety with their problem
noise and may actively avoid these environments and this may lead to
social isolation. In the majority of decreased sound tolerance cases,
the aetiology of hyperacusis is unknown.
Evaluation:
A good
clinical evaluation is required to obtain as much information about the
different aspects of the decreased sound tolerance. It is recommended
that a full medical history be taken in addition to questions that will
help define the factors relating to the decreased sound tolerance and
provide a differential diagnosis. The types of sounds that cause a
negative reaction, the loudness of these sounds, explicit details of
the actual negative effect and any coping mechanisms. Sometimes a diary
recording symptoms and severity (on a scale of 1-10 for example) is
useful, especially for longitudinal study.
The clinical history may provide some important clues about the
aetiology of the decreased sound tolerance, such as exposure to loud
noise or viral illnesses. It should be noted that anxiety, depression,
concentration or sleep issues are frequently co-morbidities.
A full ENT examination should be undertaken with otoscopy,
tympanometry, audiology and vestibular assessment for balance/vertigo
problems. Temporomandibular dysfunction should also be ruled out. Blood
tests will be useful to screen for infections or endocrinological
dysfunction. Brain MRI or temporal CT may be indicated.
While there is no clearly accepted 'consensus' method for the
evaluation of decreased sound tolerance, some people advocate assessing
loudness discomfort levels (LDLs) to provide a reasonable estimation of
the problem. However, this may also have a detrimental effect on the
subject with decreased sound tolerance and may make them anxious.
If LDL’s are to be advocated, then the subject should be fully aware of
testing procedure and if possible have full control over the maximal
sound level to which they will be exposed.
Treatment:
Historically,
advice offered to those who insisted upon help was to
'use ear plugs,' or 'learn to live with it.' Even though the aetiology
is largely unknown there are some options, however,
misophonic/phonophobic components (See below for definition) are
unlikely be removed by desensitization and a separate approach needs to
be implemented.
Subjects with hyperacusis often suffer from a lack of understanding
from others as their condition is not visible and is subjective.
Hyperacusis can have an impact on a subjects overall wellbeing and may
affect sleep, concentration, work performance and life in general.
Therefore, good communication with a clinician that can offer good
explanation of the condition will reassure the patient that they have a
recognised problem, this will help to alleviate some anxiety and
reassure them that they are believed and understood.
This will then encourage the subject to be more forthcoming with
information regarding specific behaviours and emotions when exposed to
their trigger noise. They may be more likely to express repressed
anxieties. The physical occurrence of pain with noise exposure should
be acknowledged, even though the condition may be maintained by
anxiety. Assume that any noise which is seen to be aversive is also
uncomfortable and work to break down the fear association.
Treatment
Options:
There
are three main ways in which it was proposed to treat hyperacusis, two
are diametrically opposed to each other and the other has limited
clinical success in only specific subjects with tinnitus.
Sound
Desensitisation
The
sound desensitisation approach has a more evidence-based success with
the treatment of hyperacusis especially when used in conjunction with
Cognitive Behaviour Therapy (CBT) and has similarities to Gradual
Immersion Therapy. This approach encourages the sufferer to listen to
barely audible noise for a set period of time each day. Over time the
loudness of the sound exposure is gradually increased, in this way the
tolerance to sound is built up and sensitivity to normal sounds should
become no longer painful over time. It is important keep the sound
signal carefully graded to be acceptable and under the control of the
listener.
The particular sounds that are chosen vary from clinic to clinic but
may be broadband noise or environmental noises. The choice of noise
will depend on if the subject is sensitive to specific noise (such as
chalk on black board) or general noise (such as aircraft/crowd noise).
The sound desensitisation protocol can take up to 12 to 18 months.
As it seems that auditory over-sensitivity is increased with
generalized stress and anxiety, it is important that anxiety issues are
addressed in parallel to this process.
Hearing
Protection
Historically
the most common approach was to advise patients to avoid
sound and use hearing protection. This was based on reasoning that
because patients became sensitive to sound this may indicate that they
are more susceptible to sound exposure (not true) and consequently need
extra protection.
Sufferers embraced this philosophy and started to protect their ears,
even to the extent of using ear plugs in quiet environments.
Unfortunately, research has shown that this approach of continually
attenuating the perception of sound through the use of earplugs results
in making the auditory system even more sensitive to sound, an outcome
known as a ‘threshold shift’. The result is that the hyperacusis is
exacerbated rather than improving the functionality of the individual.
With the advent of modern hearing protection there may be some merit in
using filtered hearing protection to attenuate very loud noise and
allow speech to be less attenuated however, there is no long term
research to validate the usefulness of these types of hearing
protection.
Pink
Noise
This
method has only limited success with hyperacusis and is more useful in
the treatment of subjects with reduced sound tolerance and tinnitus in
the form of Tinnitus Retraining Therapy (TRT). This method involves
assessing the LDL’s of the subject and then applying pink noise over a
period of 6 months or so at varying loudness levels for periods of
time, multiple times a day.
The pink noise can be delivered by miniature sound generators that look
similar to hearing aids and can be Behind-the-Ear or In-the-Canal. An
alternative method would be to obtain the pink noise on a CD or via the
internet (YouTube for example) and a set of headphones or earphones.
Other
Options
These
days most hearing aid manufacturers have applications for mobile
devices (iOS/Android) that facilitate tinnitus treatment that may
benefit those with decreased sound tolerance issues.
Other experimental treatments are available,
including biofeedback, relaxation strategies, and acupuncture. It is
important to research any hyperacusis management technique before
beginning to use it. Treatments should be personalised to the
individual. Medication is not generally a treatment for hyperacusis but
may be a part of the treatment process, helping sufferers cope with the
stress related to the disorder. Through future research, a better
understanding of the underlying causes of hyperacusis will lead to new
and better treatments.
Misophonia
(Sometimes called Annoyance Hyperacusis)
Means a
‘dislike of sound’, in misophonia subjects generally have a negative
attitude to certain sounds that is unrelated to the volume. It is
thought that the mechanisms of this reaction may be related to an
enhancement of the functional links between the auditory and limbic
systems or may be at the cognitive/subconscious level. Usually
misophonia is distinguished by an individual who reacts strongly to
soft sounds and is sometimes further affected by seeing the source of
the offending sound. This reaction could be irritation, dislike or even
induce some anxiety.
Common examples of misophonia would include the sound of people eating,
sniffing, repetitive sounds or certain repeated environmental sounds
like a door rattling. There are many more examples of misophonia.
Phonophobia
(Sometimes called Fear Hyperacusis)
Meaning
a literal fear of sound. This is also an adverse emotional response
involving fear or anxiety in response to sound, again the volume of the
sound is not necessarily a factor. With phonophobia the potency of the
reaction is only partially related to the sound and is also dependent
upon the subjects’ recollection of the previous negative experience of
it. Phonophobia is thought to have more of a relationship with the
cognitive and subconscious aspects of a subject. The fear/anxiety from
sound can be experienced in real time or from the expected near future
occurrence of the sound.
Some examples of phonophobia would be gunshot, the sound of a potential
threat or a sound that brought a negative experience previously such as
bad news delivered over the telephone and a resultant fear/anxiousness
of telephones ringing.
Hypersensitivity
(of Certain Frequencies)
The
term hypersensitivity is used when an individual, who is usually born
sound sensitive, is less tolerant to sounds but the sensitivity is only
to specific frequencies at a typically loud level (above 70 dB) as
opposed to hyperacusis. These subjects can usually tolerate most sounds
at normal or even loud levels but have difficulty with a certain
problem frequency or frequencies. These problem frequencies can be
identified or narrowed down by audiometric testing or by careful
questioning.
Autistic children are good examples of this as they can tolerate sound
at normal levels or even loud volumes but at some frequencies, the
sound is difficult for them to tolerate. Some organisations advocate
treatment with auditory integration therapy (AIT), however there is
insufficient evidence to support its use. AIT takes regular music
and filters out the problem frequencies through a special machine
called an audiokinetron (http://www.drguyberard.com/). Somehow, this
therapy allegedly seems to 'retune' their ears and normalizes their
hearing tolerances. The music is listened to at decibel levels
which can reach up to 90 decibels.
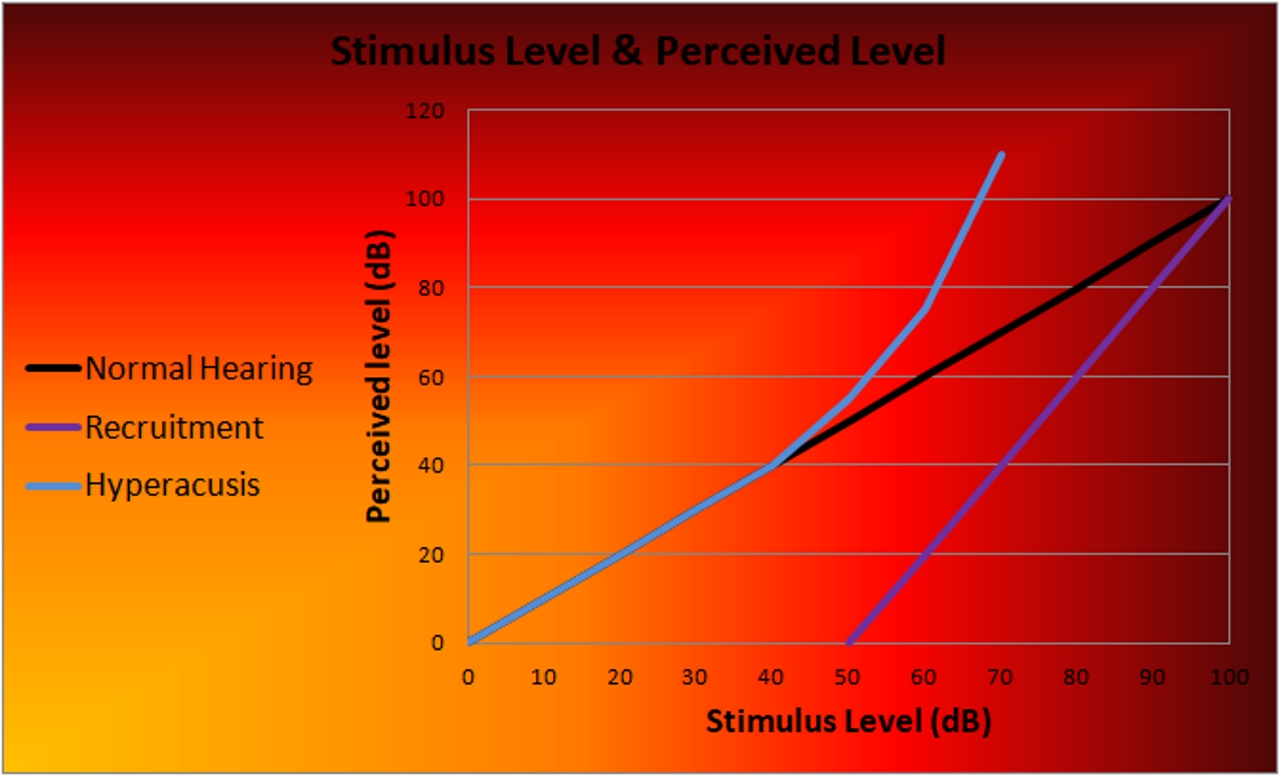
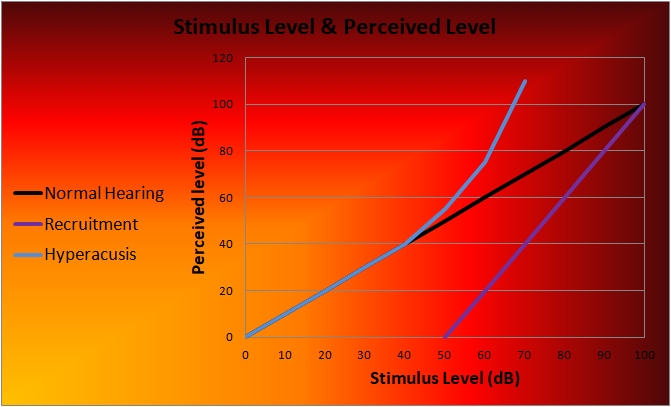
Recruitment
(Loudness)
Loudness
recruitment is usually related to cochlear impairment or damage with a
resultant hearing loss. The term refers to the subjective perception of
sounds becoming disproportionately louder with increasing sound level.
So even though there is only a small increase in the noise levels,
sound may seem much louder and it can distort and cause discomfort.
This problem can arise over numerous frequencies or at a very few,
usually high frequency ones due to the hearing loss caused by the
cochlear damage.
Although the exact mechanism behind recruitment is not fully
understood, the theory behind this condition relates to hair cells
within the cochlea that are adjacent to damaged hair cells and these
are ‘recruited’ to respond (or hear) to the frequency the damaged hair
cells were meant to respond to in addition to their own specific
frequency. This results in ‘over stimulation’ of the working hair cells
and the perceived sound processed in the brain is louder. Put another
way the ‘recruited’ hair cells still function in their original
critical frequency bands and also in the adjacent ones that they have
been recruited into.
This condition manifests commonly when people with cochlear hearing
loss ask you to speak up as they cannot hear you and then complain that
there is no need to shout.
Autophony
This
where a person’s own voice is perceived to themselves as
disproportionately loud, it is sometimes echoic or booming. This
commonly caused by an unusually large or temporarily enlarged
Eustachian tube so the sound of one’s voice travels directly into the
middle ear.
Dysacusis
The
simple definition of this term is dysfunction of hearing. This is more
often related to a processing issue with a person’s inability to
comprehend sound due to sound distortion in frequency or intensity.
This condition is usually a symptom of hearing loss through aging or
disease.
Usefull
Links:
|
|